
Can kidney disease be inherited?
The relationship between kidney disease and children


One of the most frequently asked doctors by patients with kidney disease may be this concern: "Will my kidney disease be passed on to my children? Will it be transmitted to relatives?"
Nephrologists often encounter patients with a family history of chronic kidney disease (CKD), which means that families with CKD have common genetic predispositions, or social and environmental factors.
So, is it because of genetic or environmental factors in familial CKD patients? To what extent can these two factors lead to the occurrence of CKD? How to use this information to improve CKD management?
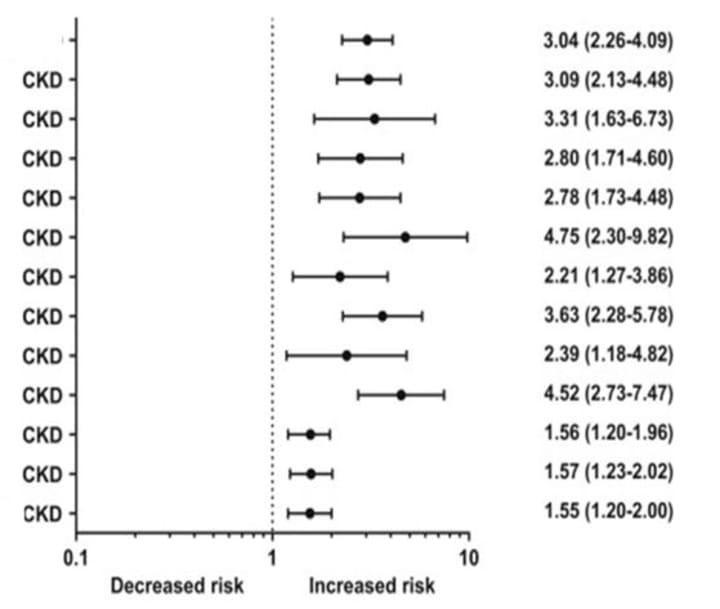
The researchers conducted a cross-sectional study to evaluate the family clustering of CKD and the heritability of related indicators and traits. Two of the results are particularly alarming. Compared with the general population, the first-degree relatives (parents, children, and siblings of the same parents) of CKD patients have a three-fold increase in the risk of CKD (RRR, 3.04 [95% CI, 2.26-4.09])
The spouse of CKD patients also increased the risk of CKD by 56% (RRR, 1.56 [95% CI, 1.20-2.00])
In addition, studies have found that these indicators related to renal function and CKD: uric acid level; eGFR; serum creatinine, urea, serum potassium, calcium, and sodium concentrations; 24-hour urine albumin excretion; and urine albumin-creatinine ratio. Obviously hereditary.
Research plan and results
This study included 155,911 general populations in Europe, covering three-generation families, and assessed the familial clustering and influencing factors of CKD. The main result of the study is the occurrence of CKD, which is defined as glomerular filtration rate (eGFR) <60mL/min/1.73m2, estimated by the creatinine equation. In the sub-samples with urine albumin concentration (n=59,943), urine albumin excretion was expressed as urine albumin excretion rate (UAE) or urine albumin-creatinine ratio (UACR) per 24 hours.
Known CKD risk factors (body mass index [BMI], hypertension, diabetes, hypercholesterolemia, smoking status, and cardiovascular history) were used as covariates.
It was found that among the 155,911 participants with eGFR data, the prevalence of CKD was 1.19%. In families with at least one CKD patient, the prevalence of CKD is 5.8%.
The CKD risk of the first-degree relatives of CKD patients is 3 times the risk of the total sample (RRR, 3.04 [95% CI, 2.26 to 4.09). The risk of CKD in the spouse of CKD patients is also higher (RRR, 1.56 [95% CI, 1.20-1.96]), indicating that there are common environmental factors or a preference for sexual partner choice (for factors such as smoking, height, BMI, and education level) And these are the potential influencing factors of CKD).
Among the related parameters of CKD, the heritability rates of eGFR, UAE and UACR were 44%, 20% and 18%, respectively. Estimates for serum urea, creatinine, and uric acid are 31%, 37%, and 48%, respectively, while estimates for serum electrolytes are between 22% and 28%.
In conclusion
The genetic factors of CKD include single-gene disease and polygenic risk. Recent clinical sequencing studies have detected diagnostic variants in 10% to 25% of patients in various CKD populations. In addition to single-gene diseases, polygenic risks--the cumulative effects of common genetic variants that affect lesser--have been shown to affect some glomerulonephropathy.
On the other hand, many environmental susceptibility factors, such as diet, lifestyle, toxin exposure (such as second-hand smoke) or infectious diseases, may cause familial influence and promote the occurrence of CKD.
In this large family study, the family history of CKD was closely related to the increased risk of CKD. Kidney traits and related biomarkers are moderately to highly heritable, and the susceptibility of family members, especially spouses, is increased. These results indicate that genetic factors or common environmental factors play an important role in the risk of CKD.
How should we understand and use these results?
The first major finding is that first-degree relatives of CKD patients have a three-fold higher risk of CKD, even in the early stages of CKD, and exclude BMI, hypertension, diabetes, hypercholesterolemia, cardiovascular history, and smoking status The same is true for other factors. CKD is usually a silent disease, and many kidney patients may not go to the doctor until late. In the future, when assessing the risk of kidney disease, family history data can be included in the risk calculation to increase the accuracy of the assessment and early identification and discovery.
The second major finding is to confirm the high heritability of eGFR and other CKD-related parameters. The recent large-scale GWAS has discovered hundreds of common variants related to CKD risk and renal function indicators. By calculating the polygenic risk score, which combines the weighted sum of all risk variants of the entire genome, the estimation of heritability has been significantly improved. . Whole genome sequencing can be performed on large CKD populations to comprehensively assess common and rare variants associated with CKD.
Finally, the “hereditary gap” and the higher risk of finding a spouse to develop CKD indicate that there is a need to better assess the environmental risk factors of kidney disease.
In short, this study proves the family aggregation of CKD in the general population, supports the influence of genetics and environment on CKD, and can ultimately guide clinicians to better refer to family factors, assess potential kidney disease risk factors, and improve patient management And results.
About the Creator
Keep reading
More stories from writers in Longevity and other communities.
Day 4 of Quitting
If this is how sobriety feels, maybe it’s better to go through life a little buzzed… this, along with other hits like, I want to kill myself, I wish I was dead, and I’m going to throw myself off a bridge have been the only thoughts on rotation these past few days. I promise myself that if, in a month, I still feel like this (‘this’ meaning despondent, full of rage, and simultaneously numb) I can go back to smoking. Until mid-February though? Nicotine is off the table.
By sleepy drafts24 days ago in Longevity
Most People Don't Feel Unhealthy ...Until Their Body Starts Limiting Their Life
Most people don't wake up one day and feel unhealthy. That's the problem. Decline doesn't announce itself. It blends in. It feels like stress. Like being busy. Like getting older. Like a phase that will pass once things calm down.
By Destiny S. Harris2 days ago in Longevity




Comments
There are no comments for this story
Be the first to respond and start the conversation.